Human Sexual Response - Summary Section 1
Welcome to the first installment of Human Sexual Response summaries. I read this book years ago and have gone back to it many times since. However, I have never written in detail about it for the blog, which is a shame because this is a fundamental work of physiological orgasm research. Plus, I think summarizing these helps me understand and retain research information better. When I go beyond a basic summary and express my personal opinions or information outside the text, I will note that specifically, often in brackets like these [ME: …].
Masters, William and Virginia Johnson. Human Sexual Response. Little, Brown, and Company, 1966.
INTRO
The intro is 2 1/2 pages and focuses on the need for solid sex research. Masters and Johnson (M&J), the study authors, quote Dickenson from 40 years prior saying, in too many words, that sex is incredibly important to humans yet, there’s an insane squeamishness about researching it with any real seriousness…and that the human race deserves better.
M&J tell us that there is widespread need for sexual education, and in order to do that properly, there needs to be better biological, physiological understanding. However, they also note the intense moral resistance. “How can biologists, behaviorists, theologians, and educators insist in good conscience upon the continued existence of a massive state of ignorance of human sexual response, to the detriment of the well-being of millions of individuals.” (p. vi-vii)
They speak of the researchers before them that tried to open the door on this type of research, sometimes to get is slammed back on their careers. They note that Kinsey’s biggest legacy may be that he kept his foot in the door “despite counter-pressures that would have destroyed a lesser man.” (p. vii)
Overall, to me this is M&J replying to the moralist objections to their work - as a preemptive move for the future of the research, but also for the future of their own careers. I think it’s easy to forget that this was a much riskier endeavor at that time than we can really imagine right now. They are also simply giving the context about why this is worthwhile, which is a sensible opening to communicating one’s research. It ends with, “This text represents the first step, a faltering step at best, but at least a first step toward an open-door policy. The door of investigative objectivity must not be closed again.” (p.vii)
I note that last line, because in my view, that door was unfortunately closed, and is still closed. Yes, there is sex research going on, but there has never been a study directly observing the physical nature of arousal and orgasm on anywhere near the scale of this one. Granted, it may have something to do with M&J themselves, given that they sort of fell apart over the years, and Virginal Johnson ended up destroying almost all their primary research. However, the other part is just that the appetite for funding this type of research seems to have waned - particularly in the United States. Ask Nicole Prause or any other American that has looked for funding and ethical permissions from their institutions. It’s incredibly hard to almost impossible from my outside understanding.
All that to say, the state of research and cultural understanding on a physiological level of the female orgasm has sadly not grown significantly past the point after this research was released in 1966, 58 years ago from the time I’m writing this.
SECTION 1: RESEARCH IN SEXUAL RESPONSE
CHAPTER 1: THE SEXUAL RESPONSE CYCLE
The investigation into the anatomy and physiology of human sexual response began in 1954 within the framework of the Department of Obstetrics and Gynecology of Washington University School of Medicine. In 1959, a research program in problems of human sexual inadequacy was established. In 1964, the programs continued as the Reproductive Biology Research Foundation. [ME: AKA - they started researching in St. Louis at Washington University where Masters was a highly regarded Obstetrician. They eventually started also doing therapeutic research for people with sexual problems, and that research I assume became the basis for their next book, Human Sexual Inadequacy. Then in ‘64, they got their own funding (for funding reasons, but also I believe morally the University wanted to be disconnected), broke from Washington University and became their own institute.]
Kinsey created a “monumental compilation of statistics,” for human sexual behavior based on comprehensive surveys. However, these weren’t designed to understand physiological or psychological response to sexual stimulus. In fact, M&J believe that they cannot be understood and sexual inadequacy cannot be successfully treated until 2 questions are answered, “What physical reactions develop as the human male and female respond to effective sexual stimulation?” and “Why do men and women behave as they do when responding to effective sexual stimulation?” They then tell us their reason for this research, “The current study of human sexual response has been designed to create a foundation of basic scientific information from which definitive answers can be developed to these multifaceted problems.” (p. 4)
The techniques they use for defining and describing the body during the sexual response cycle, “have been primarily those of direct observation and physical measurement.” Since humans aren’t super objective, even if well trained, “reliability of reporting has been supported by many of the accepted techniques of physiological measurement and the frequent use of color cinematic recording in all phases of the sexual response cycle.” (p. 4)
The have broken the human sexual response cycle into 4 phases: Excitement, Plateau, Orgasmic, and Resolution. These help to create a framework in which to discuss the physiological qualities one goes through, but these phases are certainly not to be seen as clear-cut physiological truisms.
Male sexual response cycle can be described in the following diagram. There are many variations among the male cycles, but since they are largely related to duration, rather than intensity, they would be less informative and more repetitive. Females also had many varieties, but they can be summarized with the 3 types in the 2nd diagram below. Both intensity and duration were discerning factors for the females. [ME: it should be noted that since this work, men have been physically recorded having multiple orgasms, like shown below in the female cycles, when the ejaculation was held off.]

Figure 1-1 The male sexual response cycle (p.5) From 'Human Sexual Response' (1966) by W. Masters and V. Johnson
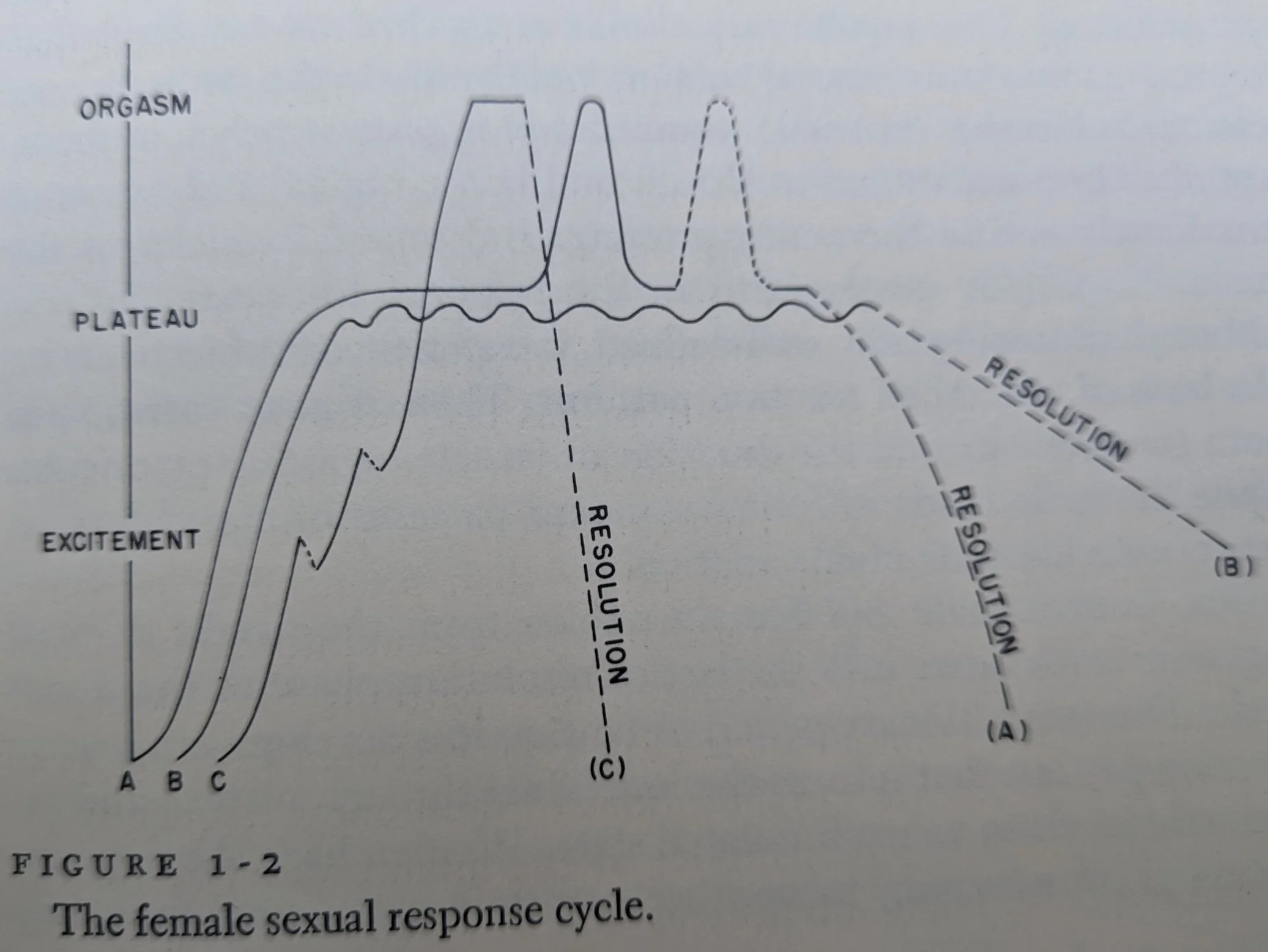
Figure 1-2 The female sexual response cycle (p.5) From 'Human Sexual Response' (1966) by W. Masters and V. Johnson
EXCITEMENT
develops from any physical or mental stimulation - quite individual.
the stimulation, if adequate for individual needs can extend the response, and the intensity of response can increase quite rapidly; if it is physically or psychologically objectionable, it can greatly slow the response or completely stop it.
This and the last phase take up the largest amount of time in the total cycle.
PLATEAU
Will move into this phase if effective sexual stimulation is continued
“sexual tensions are intensified and subsequently reach the the extreme level from which the individual ultimately may move to orgasm.” (p.6)
duration of this level depends a lot on how effective the stimulus is, as well as the individuals drive towards orgasm.
If the stimulus isn’t adequate, the person’s interest is inadequate, or all the stimulus is withdrawn, the person won’t achieve orgasmic release and the sexual tension will “drop slowly from plateau-level tension levels into an excessively prolonged resolution phase.” (p.6)
ORGASM
“The orgasmic phase is limited to those few seconds during which the vasoconcentration and myotonia developed from sexual stimuli are released.” 9p.6) [ME: AKA when all the blood pooling and muscle tension built up during arousal is suddenly released]
It’s an involuntary climax and it will be reached at any level of arousal that represents the max level for that particular occasion.
The subjective (or sensual) awareness of the orgasm is pelvic in focus (clitoral body, vagina, uterus, penis prostate, seminal vesicles).
“Total body involvement…although physiologically well defined, is experienced subjectively on the basis of individual reaction patterns. There is great variation in both intensity and the duration of the female orgasmic experience, while the male tends to follow standard patterns of ejaculatory reaction with less individual variation.” (p.6)
RESOLUTION
“This involuntary period of tension loss develops as a reverse reaction pattern that returns the individual through plateau and excitement levels to an unstimulated state.” (p.6)
Women can potentially return to orgasm from any point in the resolution phase if effective stimulation is started. This capability for multiple orgasm is evident particularly if restimulation starts at a plateau tension level.
For men, a refractory period before another orgasm may last as long as until tension levels are back at a lower excitement level. After that, restimulation to higher levels of sexual tension are possible.
“With few exceptions, the ability of the male to respond to restimulation is much slower than that of the female.” (p.7)
“The physiological residuals of sexual tension usually are dissipated slowly in both the male and female unless an overwhelming orgasmic release has been experienced.” (p.70
OVERALL
The basic physiologic responses in humans are twofold:
Primary reaction - widescale vasocongestions (aka - swelling of bodily tissue caused by increased vascular blood flow).
Secondary reaction - Myotonia or “generalized increase in muscle tension” (reflected by voluntary or involuntary muscle contraction)
Most severe vasocongestion and myotonia are in the plateau and orgasm phases
Obviously, there are some difference related to having different body parts and some variations that can be generalized between the sexes. “However, again and again attention will be drawn to direct parallels in human sexual response that exist to a degree never previously appreciated. Attempt to answer the challenge inherent in the question, ‘What do men and women do in response to effective sexual stimulation?’, have emphasized the similarities, not the differences, in the anatomy and physiology of human sexual response.” (p.8 - emphasis in original quote)
Why men and women respond the way they do is not answered in this research. The study population is not representative enough. There is some behavioral data gathered that will be presented as a contribution to understanding, but the prejudiced source of this information must always ben kept in mind. M&J do believe that until there is better behavioral information, this is at least worth some value.
They end this with, “Such data only will become available as the mores of our society come to accept objective research in human sexuality.” (p.8) [ME: we ain’t there yet, but here’s to the future!]
CHAPTER 2: THE RESEARCH POPULATION
M&J start off quickly by acknowledging that previous research has shown a bias in study subject selection; something that is unfortunately part of any “attempt to investigate biologic or behavioral facets of human sexual response,” (P.9) and that their research is no exception.
They note that they were concerned about the possibility of influence on sexual response from things such as the artificial atmosphere of the research laboratory and people’s natural anxiety about anonymity and about sexual performance. Countermeasures for problems related to this type of investigation were taken whenever possible to “improve the sociologic, psychological, and physiological integrity of the recorded data.” They will also attempt “to emphasize in context inadequacies of experimental control.” (P.10)
First the researchers focused on developing “effective techniques of interrogation, observation, and physical recording.” This was done largely with the help of prostitutes. 118 female and 27 males “contributed their sociosexual, occupational, and medical histories to the study.” (P.10)
Of those, 8 women and 3 men were selected for anatomical and physiological testing. They also helped out with the trial and error period for the investigative techniques that would eventually be used in this study. Data from this group is not included in this study’s results. The reasons given are that it is a migratory group that is hard to follow long term and also that the various pathologies of their reproductive organs may not be a good baseline of anatomical ‘normalcy'. [ME: but I mean, I think the real reason is because people would give them shit and not respect their work if it had prostitutes in it. In fact I’ve had established researchers specifically use prostitute involvement in this study to discount it…even though they were not even used in this study.]
From there the next step was getting study subjects and integrating them into the study design. They worried early on that they wouldn’t have access to study subjects from more conservative backgrounds, but they found that to be entirely false.
Subjects:
Largely related to a metropolitan university-hospital complex [ME: aka Washington University in St. Louis]
many people from the upper socioeconomic and intellectual community
married couples recruited from the hospital with various sexual or fertility issues. They represented a more diverse populations.
As the study progresses over the years, a diverse set of people also began volunteering
There was a lot of selectivity:
an initial interview ensured willingness to participate, facility of sexual responsiveness, and ability to communicate about their sexual response in detail
physical exam to ensure the reproductive organs were normal
Socially abnormal people or those with very abnormal reproductive organs were mostly excluded. However some normally occurring variants were intentionally included:
In the female population: prolapsed bladder, prolapsed urethra, a prolapse of the rectum into the back vaginal wall, uterine fibroids, tilted uterus, pregnancy-induced pelvic and labial varicose veins, pelvic endometriosis
In the male population: a benign prostate enlargement, atrophy of one testicle, an undescended testicle, abdominal hernia, and a large symptomatic varicose vein
19 female and 6 males had experienced major pelvic surgery
Only 35 males were uncircumcised
Homosexual activity in both sexes were recorded, but are not included in this study. There is not enough data yet.
The reported subject data (age, education…) represents the person at the time they started in the study
382 females, ages 18-78 with 84% between 18-40, were involved in the study (out of 1,238 interviewed). Females made up the majority of the study-subject population over the years
312 males, ages 21-89 with 74% between 18-40, were involved in the study (out of 1,308 interviewed). These are men that participated in the study at least 1 time
Subjects skewed towards college educated and white. Only 11 black couples were included and 2 single black women for special studies; one was without ovaries and the other had an artificial vagina.
There were some participants in specialize study groups
7 women with artificial vaginas
6 women in late stage pregnancy (and about 111 more that only answered questions of a behavioral nature)
34 females and 39 males between 51 and 89 years of age
General Study Considerations
There was no accurate account of the number of sexual response cycles experienced in the lab during this study, but a conservative estimate is 7,500 female cycles and 2,500 male cycles.
There was an investigation early on to compare sexual response patterns between married couples and unmarried participants. This attempt at experimental control was “abandoned as soon as it was established unequivocally that there is no difference in the anatomy and physiology of human sexual response regardless of marital status.”
It would be financially impossible to maintain the same subject group for all the years of the study, so some have only participated once and other couples have been involved for years (these people were followed partially to investigate whether years of sexual performance in the artificial lab environment changed their basic sexual patterns at all)
There was sexual behavior information gathered during detailed selection interviews, but it was decided NOT to statistically analyze and include it except in some general discussion. Compared to extensive data gathered by Kinsey, the data gathered in this study is meager, and it would not be an adequate follow-up study.
The important and unique aspect of this study is “the opportunity created by the research environment to observe, to record, and to evaluate the patterns of physiological and psychologic response to effective sexual stimulation…to a degree never before possible previously in a medical or behavioral environment.” (p.20)
“It constantly should be borne in mind that the primary research interest has been concentrated quite literally upon what men and women do in response to effective sexual stimulation, and why they do it, rather than on what people say they do or even think their sexual reactions and experiences might be” (p.20) [Me: I mean, yes. I love that shit]
Types of sexual encounters recorded and observed in this study: manual and mechanical manipulation, hetero p-in-V sex with the dude on top, dude on top with the lady’s knees to chest, and woman on top positions; and for female subjects, intercourse with a moving dildo machine while on her back with legs normal and also knee to chest.
“No study subject has been able to fantasize to orgasm under observation”
The Moving Dildo Machine
Why was this created?
“it provides opportunity for observations and recording of intravaginal physiologic response to sexual stimuli” (p.21)
helps establish effectiveness of contraceptives without years of field trials
“artificial coital techniques are used clinically to replace surgery in the creation of artificial vaginas in women born with vaginal agenesis” (p.21)
created by radiophysicists; plastic and created with same optics as plate glass; cold-light illumination allows observation and recording without distortion [ME: during thrusting], the rate of thrust and depth can be controlled fully by participant
Participants first had a period of orientation to the machine
“Suffice it to say that intravaginal physiologic response corresponds with previously established response patterns observed and recorded during hundreds of cycles in response to auto manipulation.” (p.21-22) …despite the use of such an artificial device.
The Study introduction process
Both a male and female researcher were present for interviews. This oriented the participant to feel comfortable with both sexes involved in all aspects of the study and establish a non-judgmental environment Plus, there is research suggesting having both sexes present elicits more accurate answers from participants on question with a sexual element
A tour and explanation of what would happen is given, then the subject is asked to engage in sexual activity in the lab privately and then later with the researcher close by
The subjects are not introduced to the full team and did not start participation in the study until they were fully acclimated to the lab environment.